Gastrinoma Explained: Symptoms and Key Facts

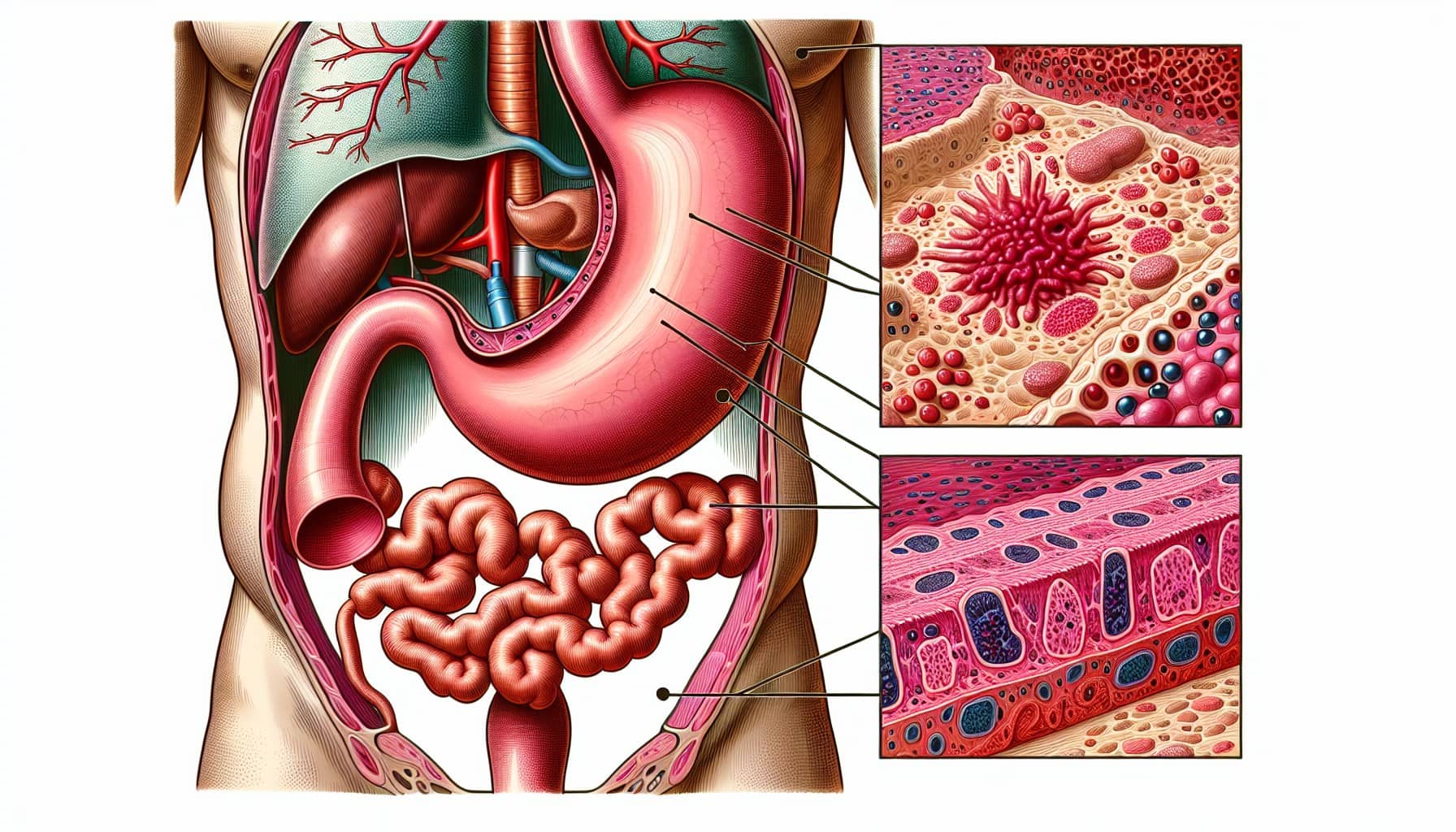
Gastrinoma is a rare type of neuroendocrine tumor that causes your body to produce too much gastrin, a hormone responsible for stimulating gastric acid. This excessive acid can lead to severe digestive issues. These tumors typically develop in the pancreas or the duodenum, the first part of your small intestine. While gastrinomas are less common than other gastrointestinal cancers, they can significantly impact your health.
The pancreas and duodenum differ in how gastrinomas behave. For example:
Gastrinoma Origin | Characteristics | Prevalence Insights |
|---|---|---|
Pancreas | Larger than 1 cm, higher risk for liver metastases | Rare in MEN-1 patients |
Duodenum | Usually smaller, lower risk for metastasis | More common than pancreatic gastrinomas |
Gastrinoma is also closely linked to Zollinger-Ellison syndrome, a condition that causes recurring ulcers and other complications due to high acid levels. Early recognition of symptoms can help you manage this condition effectively.
Key Takeaways
Gastrinoma is a rare growth that makes too much gastrin. This causes high stomach acid and digestion problems.
Usual symptoms are belly pain, long-lasting diarrhea, and heartburn. See a doctor if these symptoms don’t go away.
Surgery to remove the tumor is the best way to cure it, especially if found early.
Regular check-ups are important to control gastrinoma and avoid problems.
Changing habits, like eating smaller meals and not lifting heavy things, can help people feel better.
What Is Gastrinoma?
Definition and Characteristics
Gastrinoma is a type of neuroendocrine tumor that causes your body to produce excessive amounts of gastrin, a hormone that stimulates gastric acid production. This overproduction of acid can lead to severe digestive issues, including ulcers and chronic diarrhea. Gastrinomas are most commonly found in the pancreas or duodenum, but they can also occur in other parts of the body.
These tumors differ from other neuroendocrine tumors in several ways. For example:
Characteristic | Gastric Gastrinomas | Duodenal Gastrinomas | Pancreatic Gastrinomas |
|---|---|---|---|
Age of Patients | Older | Younger | Varies |
Gastrin Levels | Higher | Lower | Varies |
Tumor Size | Smaller | Larger | Varies |
Differentiation Grade | Lower | Higher | Varies |
Recurrence Rate | 80% | Lower | Varies |
Lymph Node Involvement | Less Common | More Common | Varies |
Mortality Rate with Liver Metastasis | 80% | N/A | N/A |
Understanding these characteristics can help you recognize how gastrinoma behaves and why early diagnosis is crucial.
How Gastrinoma Impacts the Body
When a gastrinoma develops, it triggers excessive gastrin production. This leads to several physiological changes in your body, including:
Increased secretion of hydrochloric acid (HCl).
Hyperplasia of parietal cells in the stomach lining.
Hyperperistalsis, or increased movement in the digestive tract.
Damage to the small intestine, which can cause symptoms like abdominal pain, diarrhea, and ulcers.
These changes can disrupt your digestive system and significantly affect your quality of life.
Types of Gastrinoma
Sporadic Gastrinoma
Sporadic gastrinomas account for 75-80% of cases. These tumors are not linked to genetic conditions and typically occur as isolated growths. They can develop in the pancreas or duodenum and often produce symptoms related to high acid levels.
Gastrinoma in MEN1 (Multiple Endocrine Neoplasia Type 1)
About 20-25% of gastrinomas are associated with MEN1, a genetic condition that causes tumors in multiple endocrine glands. If you have MEN1, you may develop gastrinomas alongside other tumors, such as those in the parathyroid glands or pituitary gland. These gastrinomas often occur in clusters and may require specialized treatment.
Symptoms of Gastrinoma
Understanding the symptoms of gastrinoma can help you recognize the condition early and seek timely medical care. Symptoms vary in severity, ranging from common digestive issues to life-threatening complications.
Common Symptoms
Abdominal Pain
Abdominal pain is one of the most frequently reported symptoms of gastrinoma. You may feel a persistent or recurring ache in your upper abdomen. This discomfort often worsens after eating due to the excessive acid production caused by the tumor.
Chronic Diarrhea
Chronic diarrhea is another hallmark symptom. The high levels of gastric acid can irritate your intestines, leading to frequent, watery stools. In some cases, you might notice fatty stools (steatorrhea), which occur when your body struggles to absorb fats properly.
Acid Reflux or Heartburn
Excessive gastric acid can also cause acid reflux or heartburn. You may experience a burning sensation in your chest or throat, especially after meals. Over time, untreated acid reflux can lead to complications like esophagitis or Barrett's esophagus.
Severe Symptoms
Gastrointestinal Bleeding
Gastrinomas can cause ulcers that bleed into your digestive tract. You might notice black, tarry stools or vomit that resembles coffee grounds. These signs indicate internal bleeding and require immediate medical attention.
Treatment-Resistant Ulcers
Peptic ulcers caused by gastrinoma often resist standard treatments. If you have recurring ulcers that don’t heal despite medication, it could be a sign of excessive acid production linked to gastrinoma.
When to Seek Medical Help
You should consult a healthcare provider if you experience persistent symptoms like abdominal pain, chronic diarrhea, or acid reflux. Seek immediate help if you notice alarming signs such as gastrointestinal bleeding, unexplained weight loss, or vomiting. These symptoms may indicate advanced complications that need urgent care.
Tip: Early diagnosis and treatment can significantly improve your quality of life and prevent severe complications.
Causes and Risk Factors of Gastrinoma
Causes
Genetic Mutations
Genetic mutations play a significant role in the development of gastrinoma. One of the most common mutations involves the MEN1 gene, which is linked to Multiple Endocrine Neoplasia Type 1 (MEN1). This inherited disorder increases your risk of developing gastrinomas and other neuroendocrine tumors. While some gastrinomas occur sporadically, genetic predispositions may also contribute to their formation.
Genetic Mutation | Association with Gastrinoma |
|---|---|
MEN1 | 25-30% of gastrinomas are associated with this inherited disorder, increasing the risk of gastrinomas and other neuroendocrine tumors. |
Genetic Factors | Some gastrinomas may develop sporadically, but genetic predispositions could play a role in certain cases. |
Overproduction of Gastrin
Gastrinomas cause your body to produce excessive amounts of gastrin, a hormone that stimulates gastric acid secretion. This overproduction leads to high acid levels in your stomach, which can result in ulcers, abdominal pain, and other digestive issues. The exact mechanism behind this overproduction often ties back to genetic mutations or abnormal cell growth in the pancreas or duodenum.
Risk Factors
Family History of MEN1
A family history of MEN1 significantly increases your risk of developing gastrinoma. If one of your parents has MEN1, you may inherit the condition, which raises the likelihood of gastrinomas and other endocrine tumors. Additionally, a family history of gastrinoma or neuroendocrine tumors can further elevate your risk.
Age and Gender
Gastrinomas are more common in men between the ages of 30 and 50. However, they can occur at any age and affect both genders. While age and gender are not direct causes, they are important factors to consider when assessing your risk.
Note: If you have a family history of MEN1 or experience symptoms like persistent abdominal pain or chronic diarrhea, consult a healthcare provider. Early detection can improve outcomes and help manage the condition effectively.
Diagnosing Gastrinoma
Medical History and Physical Exam
Diagnosing gastrinoma begins with a detailed medical history and physical examination. Your doctor will ask about symptoms like abdominal pain, chronic diarrhea, or recurring ulcers. They may also inquire about a family history of conditions such as Multiple Endocrine Neoplasia Type 1 (MEN1). During the physical exam, your doctor might check for signs of gastrointestinal distress or complications like weight loss or anemia. These initial steps help guide further diagnostic testing.
Diagnostic Tools
Accurate diagnosis often requires specialized tools to confirm the presence of gastrinoma and assess its severity.
Blood Tests for Gastrin Levels
Blood tests measure fasting serum gastrin levels, which are typically elevated in gastrinoma. If your gastrin levels exceed 1000 pg/mL, it strongly suggests the presence of this tumor. However, for borderline cases, additional tests like the secretin stimulation test may be necessary.
Imaging Studies (CT, MRI, Endoscopic Ultrasound)
Imaging studies help locate the tumor and determine its size and spread. Common imaging techniques include:
Computed Tomography (CT): Useful for detecting tumors and assessing metastasis.
Magnetic Resonance Imaging (MRI): Effective for identifying liver metastases but less reliable for small tumors (<1 cm).
Endoscopic Ultrasound (EUS): Highly sensitive for pancreatic tumors, with accuracy rates exceeding 90%.
Sensitivity/Accuracy | Notes | |
|---|---|---|
Somatostatin receptor scintigraphy (SRS) | Most sensitive noninvasive | Useful for localizing primary tumors and metastases; false positives can occur. |
Endoscopic ultrasonography (EUS) | >90% for intrapancreatic | Effective for detecting primary tumors; less sensitive for extrapancreatic gastrinomas. |
Computed tomography (CT) | Helpful in detection | |
Magnetic resonance imaging (MRI) | Great for liver metastases | Not effective for tumors <1 cm. |
Upper endoscopy | Useful for proximal duodenal | Can localize tumors in patients with primary gastrinomas. |
Secretin Stimulation Test
This test is particularly helpful when fasting serum gastrin levels are inconclusive. During the procedure, you receive an intravenous dose of secretin. Your doctor then measures your gastrin levels at intervals to evaluate the response. A significant increase in gastrin confirms the diagnosis of gastrinoma.
Differential Diagnosis
Several conditions mimic gastrinoma symptoms, making accurate diagnosis essential. For example, peptic ulcers caused by gastrinoma can resemble those from an annular pancreas. This condition compresses the duodenum, leading to similar digestive issues. Proper differentiation ensures you receive the right treatment.
Tip: Early and precise diagnosis improves treatment outcomes and helps manage symptoms effectively.
Treatment Options for Gastrinoma

Medications
Proton Pump Inhibitors (PPIs)
PPIs are the first-line treatment for managing gastrinoma symptoms. These medications reduce stomach acid production, allowing ulcers to heal and preventing new ones from forming. Studies show that 60% of patients experience ulcer healing within two weeks, and 90-100% recover within four weeks. PPIs are highly effective and widely prescribed for symptom control.
Somatostatin Analogs
Somatostatin analogs, such as Sandostatin LAR, help regulate hormone levels in your body. These drugs can suppress gastrin secretion, reducing acid production and alleviating symptoms. In some cases, patients have shown an almost complete response to this treatment. Your doctor may recommend these medications if PPIs alone are insufficient.
Medication Type | Effectiveness Description |
|---|---|
Proton pump inhibitors | Highly effective; 60% of patients heal ulcers within 2 weeks, 90-100% within 4 weeks. |
H2-receptor antagonists | Good success rate, but treatment fails in 50% of patients. |
Chemotherapy | Reduces tumor size and improves symptoms; response rate up to 65% with specific drug combinations. |
Somatostatin analog (Sandostatin LAR) | Described to have almost complete response in a patient. |
Surgical Treatments
Tumor Removal
Surgical resection offers the best chance for a cure if the tumor is localized. Complete removal leads to a cure in 20-25% of patients. If the tumor is entirely removed, you have a greater than 90% chance of surviving 5 to 10 years. However, incomplete removal reduces the 5-year survival rate to 43% and the 10-year rate to 25%.
Debulking Surgery
If the tumor has spread, debulking surgery may help reduce its size and alleviate symptoms. While this procedure does not cure gastrinoma, it can improve your quality of life and make other treatments more effective.
Key Outcomes of Surgical Treatments:
20-year disease-related survival: 73%-88%.
10-year disease-free survival rate: 25%-50%.
Other Therapies
Chemotherapy
Chemotherapy is often used for advanced gastrinoma cases. It can shrink tumors and improve symptoms. Specific drug combinations have shown a response rate of up to 65%. This therapy is particularly useful when surgery is not an option.
Targeted Therapies
Targeted therapies focus on specific molecules involved in tumor growth. These treatments can slow disease progression and improve outcomes. Your doctor may recommend targeted therapies if other options are less effective.
Note: Treatment plans vary based on the tumor's size, location, and spread. Consult your healthcare provider to determine the best approach for your condition.
Managing Zollinger-Ellison Syndrome
Managing Zollinger-Ellison syndrome (ZES) requires a combination of medical treatments, surgical options, and collaborative care. This approach helps control symptoms, reduce complications, and improve your quality of life.
Medical Treatment
Proton pump inhibitors (PPIs) are the cornerstone of ZES management. These medications, such as omeprazole or esomeprazole, effectively suppress acid secretion by blocking the hydrogen-potassium ATPase pump in your stomach. By reducing acid levels, PPIs help heal ulcers and prevent new ones from forming. Their introduction has significantly improved symptom control and reduced the need for immediate surgery. You should work closely with your doctor to determine the right dosage and monitor your response to treatment.
Surgical Approach
Surgery may be an option if your gastrinoma is localized and can be completely removed. This curative approach offers the best chance for long-term relief. However, surgery is not always feasible, especially if the tumor has spread. In such cases, other treatments take priority. Discussing surgical options with a specialist can help you understand the potential benefits and risks.
Multidisciplinary Care
Effective management of ZES often involves a team of healthcare professionals. Gastroenterologists and surgeons collaborate to create a personalized treatment plan. Referrals to specialized centers can provide access to advanced diagnostic tools and therapies. This team-based approach ensures you receive comprehensive care tailored to your needs.
Strategy Type | Description |
|---|---|
Medical Treatment | Use of PPIs (e.g., omeprazole, esomeprazole) for symptom control and suppression of acid secretion. |
Surgical Approach | Surgery with curative intent when feasible, especially for localized gastrinoma. |
Multidisciplinary | Collaboration between gastroenterologists and surgeons, with referrals to specialized centers. |
Tip: Early and consistent management of ZES can prevent complications and improve your overall health. Always consult your healthcare provider for the best course of action.
Prognosis and Living with Gastrinoma
Prognostic Factors
Tumor Size and Location
The size and location of the tumor play a critical role in determining your prognosis. Smaller gastrinomas in the duodenum often have better outcomes compared to larger pancreatic tumors. If the tumor is localized and completely removed through surgery, you may achieve a complete cure. Surgical resection offers a five-year survival rate of 90% for localized tumors. However, larger tumors or those in challenging locations may require additional treatments, which can affect long-term outcomes.
Metastasis
Metastasis significantly impacts survival rates. If the tumor spreads to the liver, the five-year survival rate drops to 20-30%. In contrast, localized tumors or those that have only spread to nearby lymph nodes have a much higher survival rate of 90%. Early detection and treatment are crucial to prevent metastasis and improve your chances of long-term survival.
Note: Regular monitoring and timely intervention can help manage the disease effectively, even in advanced cases.
Long-Term Management
Monitoring and Follow-Up
Ongoing monitoring is essential for managing gastrinoma. You should schedule regular follow-up appointments to check for recurrence. Measuring fasting serum gastrin levels is one of the most reliable ways to detect disease activity. Imaging tests like CT scans, MRIs, or somatostatin receptor scintigraphy may also be used periodically to assess tumor growth or metastasis. Consistent follow-up care ensures that any changes in your condition are addressed promptly.
Lifestyle Adjustments
Making lifestyle changes can improve your quality of life. Adjusting your diet to include smaller, more frequent meals can help manage symptoms caused by excessive gastric acid. Avoiding strenuous activities, such as heavy lifting, may also prevent complications during recovery. These adjustments, combined with medical care, can help you maintain a better balance in daily life.
Lifestyle Change | Description |
|---|---|
Dietary Changes | Eat smaller, frequent meals to manage symptoms related to high gastric acid. |
Activity Modifications | Avoid strenuous exercise or heavy lifting during recovery. |
Tip: Collaborating with your healthcare provider can help you create a personalized plan for long-term management.
Gastrinoma is a rare neuroendocrine tumor that demands careful attention. Key points to remember include:
Surgical removal offers the best chance for a cure, though locating the tumor can be challenging.
Symptoms like abdominal pain and diarrhea often require management during treatment.
Regular follow-ups, including imaging and gastrin level checks, help monitor recurrence.
Emotional support and lifestyle changes improve coping and recovery.
Early diagnosis is vital. Untreated gastrinomas can cause severe complications, but timely surgery improves survival rates. For example:
Surgical Outcome | 5-Year Survival Rate | 10-Year Survival Rate |
|---|---|---|
Complete removal of tumor | >90% | |
Incomplete removal of tumor | 43% | 25% |
If you notice persistent symptoms, consult a healthcare provider promptly. Early action can make a significant difference.
FAQ
What is the difference between gastrinoma and Zollinger-Ellison syndrome?
Gastrinoma is a tumor that produces excessive gastrin. Zollinger-Ellison syndrome (ZES) refers to the condition caused by this overproduction, leading to high stomach acid levels. You can think of gastrinoma as the cause and ZES as the effect.
Can gastrinoma be cured completely?
Yes, surgery can cure gastrinoma if the tumor is localized and fully removed. However, if the tumor has spread, treatments focus on managing symptoms and slowing progression. Early diagnosis improves your chances of a cure.
How is gastrinoma different from other neuroendocrine tumors?
Gastrinoma specifically produces gastrin, causing high stomach acid levels. Other neuroendocrine tumors may produce different hormones or none at all. Gastrinoma often leads to digestive symptoms like ulcers and diarrhea, which are unique to its excessive acid production.
Is gastrinoma hereditary?
In some cases, yes. Gastrinoma can occur as part of Multiple Endocrine Neoplasia Type 1 (MEN1), a genetic condition. If you have a family history of MEN1, your risk of developing gastrinoma increases.
What should you do if you suspect gastrinoma?
You should consult a healthcare provider immediately. Persistent symptoms like abdominal pain, chronic diarrhea, or treatment-resistant ulcers may indicate gastrinoma. Early medical evaluation can lead to timely diagnosis and better outcomes.
Tip: Keep a record of your symptoms to share with your doctor. This helps with accurate diagnosis.
---
ℹ️ Explore more: Read our Comprehensive Guide to All Known Cancer Types for symptoms, causes, and treatments.
See Also
Essential Insights About Carcinoid Tumors You Must Understand
Key Features and Insights Into Cholangiocarcinoma Explained
Important Information About Embryonal Carcinoma You Should Know
Carcinoid Syndrome: Symptoms and Important Information Explained
Craniopharyngioma: Key Characteristics and Understanding Its Nature

© 2026 Banish Cancer. Banish Cancer is a registered non-profit organization providing evidence-based research, educational courses, and Fear Response AI support services. Reg. No: 305706884 | Address: Taikos pr. 43-603, Kaunas, Lithuania.